
Compromised: Uncovering the immune-related challenges facing people with chronic lymphocytic leukaemia
Foreword
Cast your minds back to the early stages of the COVID-19 pandemic – to the fear you may have experienced, the uncertainty and the isolation as you were locked down and were unable to meet with your friends and family. Remember being scared about the potential of catching an infection that could have serious consequences for your health, and how this affected the way you had to cope throughout the pandemic.
These feelings and challenges can be a part of the day-to-day reality for people living with chronic lymphocytic leukaemia (CLL) who are often vulnerable to infections and related complications – even in times when there is no threat from a pandemic.
Despite a compromised immune system being a key challenge for many people with CLL, patients often feel that it is not well known or understood by clinicians.[1] Information and guidelines on diagnosis and classifications other immune challenges is often not consistent and this creates a significant unmet need for people with CLL.[2] Continuing to improve both survival and quality of life for people with CLL must remain a focus in cancer treatment and care. Identifying meaningful strategies to managing immune risk is the difference between being able to live a full life and having to avoid physical interactions.
Given the spotlight the COVID-19 pandemic shone on immunocompromised people, the CLL Advocates Network (CLLAN) and AstraZeneca wanted to build on this public recognition to positively impact the care and support offered to people with CLL. I am incredibly grateful to all the individuals and organisations who have contributed to this piece of work. It is only by bringing together the insight of patient representatives and the expertise of clinicians that we can make practical and tangible recommendations that will help people with CLL to come out from behind the protective shield and live as full a life as possible.
I hope that this is a powerful and thought-provoking white paper that broadens your understanding of the unspoken experiences of people with CLL and moves you to consider your role in transforming care for people with CLL facing immune challenges.
Nick York
Working group member
Chair, CLL Advocates Network
![]()
Table of contents:
Introduction
People with CLL are particularly vulnerable to infections
How are infection risks managed in people with CLL?
How do immune-related challenges impact the day-to-day lives of people with CLL?
Prevention and monitoring have key roles to play in addressing CLL immune-related challenges
Conclusion & Key Recommendations
References
![]()
The preparation of this white paper was commissioned and funded by AstraZeneca. The themes and content of the white paper were co-developed and reviewed by CLL Advocates Network (CLLAN) and AstraZeneca. CLLAN representatives did not receive any financial compensation in relation to this white paper.
What is CLLAN?
The CLL Advocates Network (CLLAN) was founded in 2014 by representatives from Canada, Czech Republic, France, Ireland, Italy, Portugal, UK and the United States. It is hosted under the umbrella of the Leukemia Patient Advocates Foundation (LePAF), a patient-led non-profit foundation based in Switzerland acting as a legal platform for self-sustained patient advocacy initiatives. CLLAN is governed by a Steering Committee consisting of the 9 members, of whom 6 are patients and 1 is a carer. Ultimately, CLLAN’s mission is to improve Chronic Lymphocytic Leukaemia (CLL) patient outcomes.
The following principles guide CLLAN’s work:
CLLAN’s white paper working group

With thanks to:
Nick York (Chair), Pierre Aumont, Rita Christensen, Lea Koren, Jan Rynne and Raymond Vles.
The working group’s thanks also go to Professor Paul Moss, University of Birmingham (UK), and Professor Clemens-Martin Wendtner, München Klinik (Germany), who kindly acted as non-compensated reviewers of this white paper and provided input on content.
Introduction
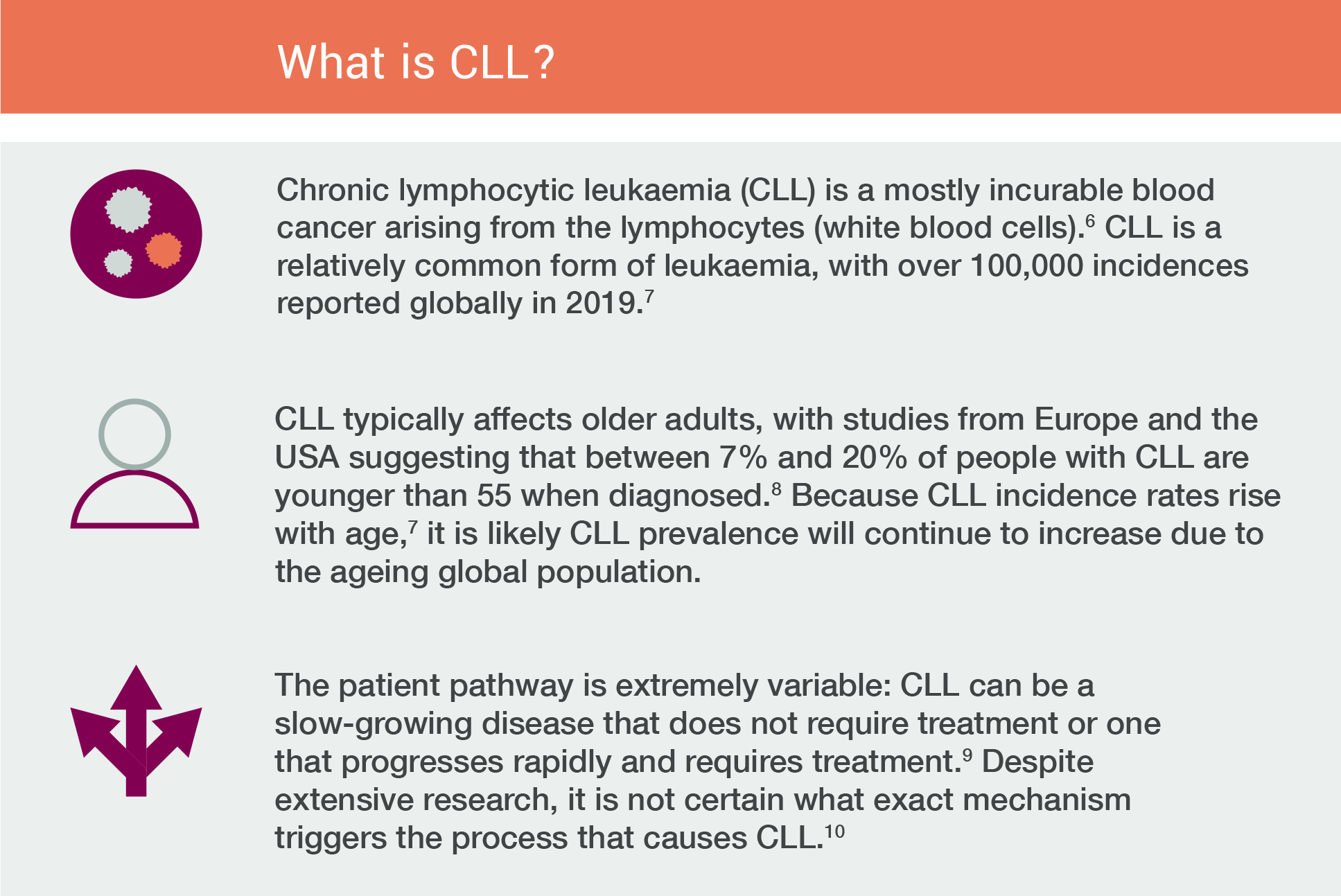
Over the past two decades, significant progress in therapies for chronic lymphocytic leukaemia has markedly improved survival rates.[3] As a result, fewer people are dying of CLL itself. The projected five-year survival of people with CLL is a promising 85%. [4]
However, despite advances in therapy, infection remains a major risk in CLL and is a key challenge in CLL management. [5] People with CLL face varied immune challenges – in addition to infections – along the patient pathway, which form a major part of managing day-to-day life with CLL. This area has long been overlooked in CLL management and care, despite infections being a leading cause of mortality in people with CLL. [3] There is currently no consensus on what ‘good’ immunocompromised management looks like for people with CLL.
The COVID-19 pandemic has shone a spotlight on the immune-related challenges that put people with blood cancer at greater risk of COVID-19 infection, and the subsequent impact on day-to-day activities and wellbeing. There is now an opportunity to expand this focus to raise awareness of immune-related complications associated with CLL that are currently both under-reported and not fully understood by patients or primary physicians.
Although the issues that come with being immunocompromised are longstanding for people with CLL, and certainly not exclusive to the pandemic, the CLL Advocates Network (CLLAN) and AstraZeneca see an opportunity to take advantage of the increased attention on immune challenges, demonstrating both available data and current information gaps, and delivering meaningful recommendations to support improvements for people with CLL. ![]()

People with CLL are particularly vulnerable to infections
People with CLL have an immune dysregulation that predominantly manifests as an increased susceptibility to infection and/or autoimmunity. [11]
This can result in a higher risk of opportunistic infections, but also increases the occurrence of secondary cancers,[12] autoimmune complications, affecting the course and management of the disease. [11,13]
Primary causes of death for people with CLL are progressive disease and infections; infections are acknowledged to be a significant cause of morbidity throughout the disease course.[15] The origin and development of infections in people with CLL can be particularly challenging to diagnose quickly and, in some cases, infections can be misinterpreted as disease progression.
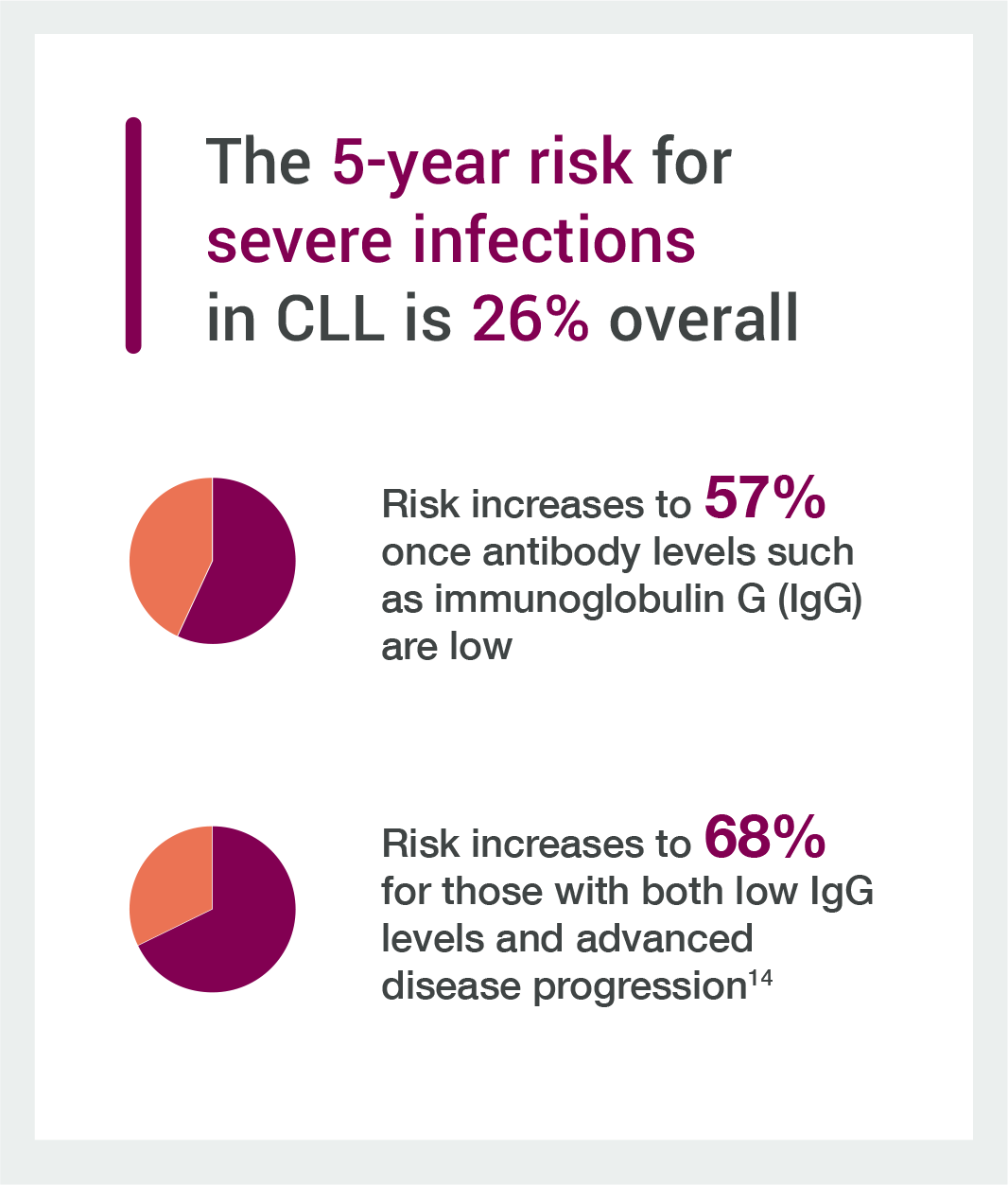
There is increased risk of severe infection due to the immunosuppression caused by the disease, and a risk of infection as a consequence of treatment. [14,16]
People with CLL have an intrinsically higher risk of community-acquired infections, often manifesting as bacterial infections of the respiratory tract, urinary tract and skin.[17] Even in people with early-stage CLL, there is evidence of decreased immune responses.[18]
However, the rate, severity and prognostic factors for infections in people with CLL prior to treatment – as well as the impact on quality of life – constitute a knowledge gap that ought to be addressed. [19]
CLL treatment can also increase the likelihood of infection, although encouragingly novel therapies are often less immunosuppressive than previous chemotherapy approaches. [20]
The experts who inputted into this White Paper noted that there can be a low awareness of immune-related challenges faced by people with CLL amongst both patients and some healthcare professionals.
If people with CLL do not have a good understanding of their disease, they are unable to seek the correct information for their condition that can help them better manage their condition. In the case of immune challenges specifically, this lack of information and understanding can have a particularly detrimental impact.
For healthcare professionals, infections should be a more central topic of conversation with patients, and momentum from the COVID-19 pandemic may enable discussion on immune-related challenges as an important topic in CLL care. Challenges related to being immunocompromised should be systematically addressed during clinical appointments, and a patient’s vaccination history for common infections should also be checked. These patient-clinician discussions should be personalised, with a focus on ensuring patient preferences are heard and that shared decisions are reached. In a similar vein, information developed by patient advocacy groups on infection management should be signposted for people with CLL.
A key challenge remains, however, that currently available clinical guidance for managing people with CLL tends not to directly address monitoring and managing immunosuppression. Guidance is also inconsistent globally; for instance, the British Society for Haematology and the German Society for Haematology and Medical Oncology (DGHO)’s guidelines for treating CLL both recognise immune-related challenges and offer recommendations in the context of supportive therapies.[21,22] Further work is required to ensure that national haematological bodies recognise and adopt similar standards of immunocompromised care; the International Workshop on CLL (iwCLL) may be well placed to develop more specific guidelines and work with national champions to ensure effective implementation.
Expert contributors also noted that the variations in CLL diagnoses and classification, coupled with limitations to cancer systems,[23] may be contributing to the lack of existing guidelines. Patient advocacy groups could have a role to play in generating this knowledge. ![]()
How are infection risks managed in people with CLL?
Therapies that support immune function, such as immunoglobulin, are common in CLL management. [14]
Hypogammaglobulinemia is a predominant inherent immune defect in CLL and can be further exacerbated by immunosuppressive treatment.[24] The severity of hypogammaglobulinemia is correlated with stage, duration of disease, and susceptibility to severe and recurrent infections. [20] Immunoglobulin levels tend to be significantly lower in people with advanced stage CLL who have received chemotherapy. [25]
Measurement of immunoglobulin levels is particularly important in those with recurrent or severe infections.[25] Both reduced and elevated immunoglobulin levels at diagnosis are independent prognostic markers for infection in CLL, with certain types of immunoglobulins (such as IgA) being more relevant as a marker of disease progression and survival.[26] Early replacement intravenous immunoglobulins can play an important role in reducing severe infections. [25]
Additionally, subcutaneous immunoglobulin therapies are becoming a more frequent choice. In comparison to IV immunoglobulin therapy, they can also facilitate higher levels of IgG (the most common antibody) and can decrease the incidence of severe infections, even during continuous CLL therapies. [27]
Ultimately, early diagnosis and intervention are crucial. A patient’s history, assessment of risk factors and assessment of antibody levels should all be carefully and regularly reviewed in order to diagnose infections and treat them effectively. [14]
However, there is variation in the clinical assessment and management of infections in people with CLL.
While some healthcare professionals conduct an immune evaluation to understand if immune protection and vaccination history are optimised, others may not.
Additionally, the level of information people with CLL are given regarding managing their immunosuppression is unclear, although it is evident that healthcare professionals are generally a key source of information for people with CLL. In one 2020 global survey of people with CLL or lymphoma, 69% of respondents stated they would first go to a doctor for information about their care. Notably, only 4% chose a nurse as their first option,[28] despite nurses often playing a key role in managing the care of chronic patients with CLL, indicating a potential need to increase communication regarding their role. Only 52% of respondents stated that they always had trust and confidence in the information given to them by nurses,[28] although it is worth noting that this figure could vary substantially depending on a country’s health system and its approach to CLL care.
Clear guidance for healthcare professionals – addressing both management and patient information provision – is vital for a more uniformed approach that can help reduce infection incidence.
Further research is needed to identify not only the optimal touchpoints within the patient pathway for information provision, but also which healthcare professionals are best suited to provide this information.
From the point of diagnosis, care should be taken when relaying information about immune-related challenges, recognising that a range of healthcare professionals may be involved in care at various points along the patient pathway. For instance, while a CLL diagnosis tends to be given by a specialist, primary physicians often play a vital role in monitoring and treating immune-related issues in people with CLL, as well as implementing preventative measures like vaccination.[29] Leukaemia Care’s Living with Leukaemia report in 2018 found that less than 50% of chronic patients surveyed felt their GP had a complete understanding of blood cancers,[30] while Lymphoma Coalition’s 2022 report found that of around 1800 people surveyed with CLL, 89% of respondents clearly understood they were being diagnosed with cancer from their initial diagnosis experience, but one in four stated they were not told the specific sub-type.[31] This indicates the need for continued work to educate and support GPs on conditions like CLL.
The role of primary physicians should be better acknowledged and signposted for people with CLL, especially in supporting vaccination and understanding lifestyle risks for infection – for instance, gardening increases risk of fungal infections and contact with children increases risk of opportunistic infections.[32,33] Collaboration between specialists and primary physicians should be commonplace in order to optimise immunocompromised management, and to ensure that primary physicians are informed of the challenges facing people with CLL. Notably, this should include education on the use of antibiotics and anti-microbials in people with CLL, which may differ from available guidance for general populations. ![]()
How do immune-related challenges impact the day-to-day lives of people with CLL?
Research suggests that CLL has a significant impact on health-related quality of life (HRQoL). [34]
Emotional functioning may also be impacted for people with CLL.[35] Nevertheless, evidence gaps remain that ultimately limit understanding of how people with CLL are affected by immune-related challenges, including in their social life and mental health.
People with CLL often lack general information on how to manage being immunocompromised and personalised information about their immunity status, which may cause distress.
CLL-specific and leukaemia patient advocacy groups develop resources that explain how CLL can lead to an immunocompromised status and, in some cases, address preventative measures and other practical patient management strategies. However, existing information on immune challenges can be hard for people with CLL to find online, possibly in part due to inconsistent categorising; for instance, some patient advocacy groups may class these issues under ‘supportive therapies’ and others, due to the COVID-19 pandemic, may host relevant resources under COVID-19-specific sections of their website.
Additionally, it is challenging to quantify the true impact of being immunocompromised on the day-to-day lives for people with CLL.
There is very limited research explicitly addressing how immune challenges impact people with CLL. Broader research exists on the impacts of CLL that can be drawn on (for instance, the psychosocial impacts of a diagnosis) [36] but currently this does not address the added complications of being immunocompromised or having to adopt various protective strategies.
Patient experience surveys tend to ask patients if they have been affected by infections or anaemia, and separately split symptoms such as pain, fatigue or swelling of lymph glands from occurrences like developing an autoimmune reaction.[37] Not grouping these symptoms together as immune-related challenges may inadvertently contribute to the limited clear evidence of the burden faced by people with CLL, as well as the low awareness of these challenges. Including a specific focus on immune challenges – whether in clinical research or in materials developed by patient advocacy groups – could help to develop a stronger evidence base.
Empowering people with CLL to take an active role in the management of their disease could also be beneficial.
Lymphoma Coalition’s 2020 Global Patient Survey reported that only 52% of people with lymphoma or CLL are involved as much as they want to be in decisions about their care and treatment.[28] There may be a gap in linking shared decision-making with educating patients to manage their infection risk. It would be valuable to have a list of questions people with CLL should ask about their immunosuppression – at different points in their patient journey – to ensure high quality conversations with their healthcare professionals. ![]()
Prevention and monitoring have key roles to play in addressing CLL immune-related challenges
Preventing infections
Consensus exists on the importance of infection prevention for people with CLL.[14,20]
This may involve options like antibiotics or vaccination. Vaccinations should be administered early in the disease course to improve the likelihood of an immune response – particularly before starting certain immunosuppressive therapies.[20] Bacterial pneumonia remains a common thoracic complication of CLL; among people with treatment-naive CLL, pneumonia is the most common serious infection.[20,38] In the case of the pneumococcal vaccine, more effective immune responses have been seen in CLL patients with early stage and stable disease. [39]
The COVID-19 pandemic has also brought greater attention to the importance of people with CLL receiving pneumococcal and seasonal flu vaccines. [20,29]
However, a lack of data remains, and urgent research is needed into the vaccination statuses of people with CLL. With a fuller evidence base, systems should be implemented to identify the vaccinations that people with CLL have received, and which vaccinations they may still require to increase their immunity against common infections. Such monitoring may also facilitate a data justification to develop more effective vaccination strategies for people with CLL who have poorer vaccine responses. [40]
As part of this, it is vital to identify the vaccination status of people with CLL from the point of initial diagnosis to fully understand their needs as their patient journey evolves. CLL Support and the UK CLL Forum have jointly created a ‘vaccination passport’ for people with CLL, which acts as both a guide, providing further information about vaccinations, and a log, for individuals to keep track of their own records.[29] By providing a standard of care for people with CLL, such patient empowerment tools have an additional benefit of mitigating variation in management and should ideally be replicated amongst other countries beyond the UK.
Shingles is of real concern for CLL patients because of their compromised immune system, often making the virus more severe and difficult to control. [41] Despite people with CLL generally having impaired responses to some vaccines, such as the COVID-19 vaccine, [42] there is a trend towards decreased infection in patients who have received the non-live shingles vaccination. [43] Additionally, post-herpetic neuralgia (PHN) is one of the prominent causes of non malignant pain in chronic leukaemia patients. [44] It can occur due to either the CLL or its treatment causing reactivation of latent varicella-zoster, requiring urgent pain management. Widespread PHN has a considerable effect on the quality of life of people with CLL. [44]
While all people with CLL should be monitored for signs of infection or other immune challenges, patients may have different risk profiles that are influenced by factors such as age, prognostic biological markers, or the stage of disease. [45,46]
Prevention strategies should be personalised to account for these factors, as should care information.
There are limited infection risk-assessment guidelines that can be easily used in clinical practice to guide more appropriate infection prophylaxis and its management, and none exist specifically for people with CLL.[47] Consolidated practice guidelines for infection prophylaxis in CLL should be developed.
Monitoring for autoimmune complications
People with CLL have a greater predisposition to develop autoimmune complications. [13]
The most common is autoimmune haemolytic anaemia (AIHA). [13] AIHA can develop in up to a third of patients with CLL during the course of their disease, and may present in up to 15% cases at diagnosis. [13] Careful monitoring is essential to ensure that a diagnosis can be made quickly. [48]
The diagnosis of AIHA can be difficult to make in the setting of CLL, and complications seem to correlate with advanced stage CLL, higher age, and poor prognostic markers. [46] It is important that personalised care and information is available for people with CLL on the topic of autoimmune complications, as factors such as age and prognostic markers may affect their likelihood.
Autoimmune thrombocytopenic purpura (AITP) may also develop and can be difficult to distinguish from bone marrow infiltration with CLL.[49] Haematologists are usually familiar with AIHA and AITP as the most common types of autoimmune cytopenia (AIC), but less so with non-hematologic AIC. [48] ![]()
The risk of severe COVID-19
CLL is associated with significant immune suppression, comorbidities, and advanced age, all of which act as compounding risk factors for severe COVID-19 infection. [49]
Blood cancers are associated with higher case fatality rates from COVID-19 than other cancers.[40] While the prevalence of COVID-19 for people with CLL is not significantly higher than seen in the general population, case fatality rates in the first wave of the pandemic were up to 16.5-fold higher than the median reported worldwide. [40]
COVID-19 prevalence may have been lower than expected for a population generally susceptible to viral infections because many people with CLL were vigilantly shielding. [50] Further research is needed to enhance knowledge of COVID-19 incidence, clinical course, and immune response to the infection and vaccination in people with CLL. This could inform the design of strategies that can improve the outcomes of patients in the future. [40]
The COVID-19 pandemic has had a significant impact on quality of life for people with CLL. [50, 51]
In people with asymptomatic CLL lacking treatment indication, continuation of the watch-and-wait strategy has been widely recommended during the pandemic, and face-to-face appointments limited where possible in order to prevent nosocomial COVID-19 infections. [52] Those on watch-and-wait ‘active management’ represent a large percentage of the CLL patient group, and data suggest that these people are at high risk despite not being in active treatment. [51] The continued need to isolate in order to avoid being infected with COVID-19 holds a substantial quality of life impact for people with CLL. [53]
While the COVID-19 pandemic has been an especially challenging time for people living with CLL, some best practice management approaches may shed light on appropriate ways to assist those living with CLL as we move beyond the pandemic. Some practical guidelines to support clinicians and people with CLL have emerged, including awareness raising initiatives for vaccination programmes for immunocompromised individuals, vaccine passports, and remote consultations to lower infection risk. [29.54] In a similar vein, patient advocacy groups around the world have issued specific advice on staying safe from COVID-19 as restrictions ease. [55] The next step here could be to ensure protocols and management approaches, as well as patient resources, move beyond COVID-19 infection and address immune challenges more broadly. [56]
It is important that patient health records identify that people with CLL are immunocompromised – albeit to varying extents – to ensure that they are able to obtain the specialist care they require, whether COVID-19-related or otherwise. Such action would also facilitate awareness of immunocompromised status amongst both patients and primary physicians.
Addressing the risk of additional cancers
Elevated risks for secondary cancer have also been reported in people with CLL, including non-melanoma skin cancer, melanoma, sarcoma, and lung, renal, and prostate cancers.[57] As the survival from better CLL disease control improves further, secondary malignancy will likely become an even more dominant factor for long-term survival for a higher proportion of patients, and it will require more focus from the CLL community. [58]
Secondary lymphoid malignancies, including Richter’s transformation, are another key secondary cancer. The prognosis for Richter’s transformation is usually very poor in people with CLL.[17] In the absence of intensive therapy, the median overall survival is short. [17]
Clinicians and pathologists must be alert towards the possibility of further malignancies in CLL patients, and be ready to conduct rapid, multidisciplinary interventions when required. Care and information should be personalised, and patients should be counselled on the benefit of cancer screening, especially skin examinations.
Indeed, skin cancers are one of the most common secondary malignancies in people with CLL, and regular skin surveillance can prevent increased mortality. [59] ![]()

Conclusion & Key Recommendations
Further research is needed to build a stronger evidence base of the immune challenges facing people with CLL. This could include:
1. Establishing the impact of vaccination status on CLL outcomes
-
- Through this, robust approaches for monitoring the vaccination status of people with CLL could be established, helping healthcare professionals to understand who needs to be vaccinated
- Vaccination data for people with CLL could also facilitate the development of specific vaccination strategies for those with poorer vaccine responses
2. Quantifying and qualifying the impact of opportunistic infections that are not treatment-related
-
- By generating data sets on non-treatment-related infections, healthcare professionals can better understand factors influencing infections prior to treatment and can implement effective and personalised management approaches
3. Identifying research needed to inform planning and clarification of protective measures for immunocompromised people
-
- Building on the momentum due to the pandemic, determining and collecting relevant data can shed further light on immune challenges facing people with CLL and allow the community to be better protected
4. Understanding how people with CLL are affected by immune-related challenges with regard to their social life and mental health
-
- Building an evidence base of the difficulties facing people with CLL can allow patient advocacy groups and healthcare professionals to identify common sore spots and gaps in information, and offer appropriate support
5. Specifically adding focus on immune challenges in CLL-specific groundwork, whether clinical research or patient experience surveys
-
- Interrogating immune challenges – and how they interact with other clinical issues – opens up future possibilities for action that can improve the lives of people with CLL
Healthcare professionals should be supported to optimally manage people with CLL facing immune challenges. This could include:
6. Creating global clinical guidance for monitoring and managing immunosuppression in people with CLL
-
- Through this, healthcare professionals can manage their patients based on specific clinical best practice for people with CLL
7. Ensuring that immunocompromised status is flagged in the patient health records of people with CLL
-
- Initiating a standardised approach to identifying immunocompromised status would mean that primary physicians are more aware of their patients’ needs, and allow people with CLL to obtain the care they require
8. Instigating education and awareness raising activities amongst healthcare professionals, especially primary physicians
-
- Raising awareness of the importance of vaccination, managing common and opportunistic infections and monitoring for potential complications (such as secondary cancers or autoimmune conditions) amongst treating healthcare professionals can facilitate improvements in quality of life for people with CLL
9. Making shared decision-making and personalised approaches commonplace in the management and care of people with CLL
-
- By considering personal choice and a patient’s level of immunosuppression, people with CLL would receive the most appropriate care in the most appropriate setting for them

People with CLL should be supported with a range of information and resources to feel empowered, regardless of any immune challenges they may be facing.
10. Creating and sharing resources to educate and empower people with CLL (such as holistic self-assessments or information on the impact of certain lifestyle choices on infection risk)
-
- Patient advocacy groups should continue to develop these materials, but it is vital that input is sought from clinicians and health system leaders in order to ensure this information is signposted to people with CLL

- Patient advocacy groups should continue to develop these materials, but it is vital that input is sought from clinicians and health system leaders in order to ensure this information is signposted to people with CLL
![]()
References
[1] Leukaemia Care. Living with Leukaemia. 2018. Available at: https://media.leukaemiacare.org.uk/wp-content/uploads/Living-with-Leukaemia-2018-Full-Report-Web-Version.pdf. Last accessed February 2023
[2] Dong Y et al. Leukemia incidence trends at the global, regional, and national level between 1990 and 2017. Exp Hematol Oncol. 2020 Jun 19;9:14.
[3] Crassini, Kyle R. et al “Immune failure, infection and survival in chronic lymphocytic leukemia.” Haematologica 103, no. 7 (2018): e329.
[4] Cancer Research UK. Survival for chronic lymphocytic leukaemia (CLL). 2021. Available at: https://www.cancerresearchuk.org/about-cancer/chronic-lymphocytic-leukaemia-cll/survival. Last accessed February 2023
[5] Andersen, Michael et al”Epidemiology of bloodstream infections in patients with chronic lymphocytic leukemia: a longitudinal nation-wide cohort study.” Leukemia 33, no. 3 (2019): 662-670.
[6] Chatzidimitriou, Anastasia et al. “Challenges and Solutions for Collecting and Analyzing Real World Data: The Eric CLL Database as an Illustrative Example.” HemaSphere 4, no. 5 (2020).
[7] Yao, Yiyi et al. “The global burden and attributable risk factors of chronic lymphocytic leukemia in 204 countries and territories from 1990 to 2019: analysis based on the global burden of disease study 2019.” Biomedical engineering online 21, no. 1 (2022): 1-22.
[8] Parikh, Sameer et al. “Chronic lymphocytic leukemia in young (≤ 55 years) patients: a comprehensive analysis of prognostic factors and outcomes.” haematologica 99, no. 1 (2014): 140.
[9] Kipps, Thomas et al. “Chronic lymphocytic leukaemia.” Nature reviews Disease primers 3, no. 1 (2017): 1-22.
[10] Mayo Clinic. Chronic lymphocytic leukemia: Overview. 2021. Available at: https://www.mayoclinic.org/diseases-conditions/chronic-lymphocytic-leukemia/symptoms-causes/syc-20352428. Last accessed February 2023
[11] Dearden, Claire. “Disease-specific complications of chronic lymphocytic leukemia.” ASH Education Program Book 2008, no. 1 (2008): 450-456.
[12] American Cancer Society. ‘Second Cancers After Chronic Lymphocytic Leukemia’. Available at: https://www.cancer.org/cancer/chronic-lymphocytic-leukemia/after-treatment/second-cancers.html#:~:text=People%20with%20CLL%20can%20get%20any%20type%20of,may%20be%20from%20some%20other%20cancer%20or%20disease. Last accessed 17.04.23
[13] Pasquale, Raffaella et al “Autoimmune Hemolytic Anemia in Chronic Lymphocytic Leukemia: A Comprehensive Review.” Cancers 13, no. 22 (2021): 5804.
[14] Grywalska, Ewelina et al. “Chronic Lymphocytic Leukemia-Induced Humoral Immunosuppression: A Systematic Review.” Cells 9, no. 11 (2020): 2398.
[15] Strati, Paolo et al. “Relationship between co‐morbidities at diagnosis, survival and ultimate cause of death in patients with chronic lymphocytic leukaemia (CLL): a prospective cohort study.” British journal of haematology 178, no. 3 (2017): 394-402.
[16] Williams, AnnaLynn et al. “Analysis of the risk of infection in patients with chronic lymphocytic leukemia in the era of novel therapies.” Leukemia & Lymphoma 59, no. 3 (2018): 625-632.
[17] Quinquenel, Anne et al. “Diagnosis and treatment of chronic lymphocytic leukemia: recommendations of the French CLL Study Group (FILO).” Hemasphere 4, no. 5 (2020).
[18] Arruga, Francesca et al. “Immune response dysfunction in chronic lymphocytic leukemia: dissecting molecular mechanisms and microenvironmental conditions.” International journal of molecular sciences 21, no. 5 (2020): 1825.
[19] Andersen, Michael et al. “Incidence and predictors of infection among patients prior to treatment of chronic lymphocytic leukemia: a Danish nationwide cohort study.” haematologica 103, no. 7 (2018): e300.
[20] Sun, Clare, and Adrian Wiestner. “Can Immunocompetence Be Restored in Chronic Lymphocytic Leukemia?.” Hematology/ Oncology Clinics 35, no. 4 (2021): 827-845.
[21] Walewska, Renata et al. “Guideline for the treatment of chronic lymphocytic leukaemia.” British journal of haematology (2022).
[22] Deutsche Gesellschaft fuer Haematologie und medizinische Onkologie. Chronische Lymphatische Leukämie
(CLL) Leitlinie, September 2020. 2020. Available at: https://www.onkopedia.com/de/onkopedia/guidelines/chronische-lymphatische-leukaemie-cll/@@guideline/html/index.html. Last accessed February 2023
[23] Dong Y et al. Leukemia incidence trends at the global, regional, and national level between 1990 and 2017. Exp Hematol Oncol. 2020 Jun 19;9:14.
[24] Abbasi, Farhad. “Infectious diseases and clinical complications during treatment in CLL.” Oppezzo P. Chronic lymphocytic leukemia. 1st edition. Rijeka, Croatia: InTech (2012): 367-382.
[25] Yokus, Osman et al. “Secondary Immunodeficiency Frequency in Patients with Chronic Lymphocytic Leukemia: The Relationship with Stage and Treatment.” International Journal of Hematology-Oncology and Stem Cell Research 16, no. 1 (2022): 14-21.
[26] Ishdorj, Ganchimeg et al. “IgA levels at diagnosis predict for infections, time to treatment, and survival in chronic lymphocytic leukemia.” Blood advances 3, no. 14 (2019): 2188-2198.
[27] Visentin, Andrea et al. “Protective role immunoglobulin replacement therapy in chronic lymphocytic leukemia: FOCUS on subcutaneous immunoglobulin formulations.” Blood 132 (2018): 4954.
[28] Lymphoma Coalition. 2020 Global Patient Survey on Lymphomas & CLL. 2020. Available at: https://lymphomacoalition.org/wp-content/uploads/LC-2020-GPS-Global-Report-Final.pdf. Last accessed February 2023
[29] CLL Support and the UK CLL Forum. Vaccination guide and log for people with CLL/SLL. 2022. Available at: https://images.cllsupport.org.uk/wp-content/uploads/2022/05/04115357/CLL-Support-Vaccination-leaflet.pdf. Last accessed February 2023
[30] Leukaemia Care. Living with Leukaemia. 2018. Available at: https://media.leukaemiacare.org.uk/wp-content/uploads/Living-with-Leukaemia-2018-Full-Report-Web-Version.pdf. Last accessed February 2023
[31] Lymphoma Coalition. Chronic lymphocytic leukaemia: Subtype report. 2022. Available at: https://lymphomacoalition.org/wp-content/uploads/2022_Lymphoma_Coalition_Report_CLL_VF_A4_Digital.pdf. Last accessed February 2023
[32] Oxford University Hospitals. Prophylaxis and Treatment of Invasive Fungal Infections in Adult Haemato-oncology patients. Department of Haemotology. Oxford University Hospitals. Available at: https://nssg.oxford-haematology.org.uk/general-clinical-management/H-94-antifungal-therapy-guidelines.pdf. Last accessed 09.03.23
[33] John C Byrd MD. Chronic Lymphocytic Leukemia: Prognostic Factors, Supportive Care Issues and Therapeutic Advances. No date. Available at: https://www.danafarbermasterclass.com/assets/files/Byrd-Website.pdf. Last accessed February 2023
[34] Waweru, Catherine et al. “Health-related quality of life and economic burden of chronic lymphocytic leukemia in the era of novel targeted agents.” Current Medical Research and Opinion 36, no. 9 (2020): 1481-1495.
[35] Goyal, Neha et al. “Cancer-specific stress and trajectories of psychological and physical functioning in patients with relapsed/refractory chronic lymphocytic leukemia.” Annals of Behavioral Medicine 52, no. 4 (2018): 287-298.
[36] Leukaemia Care. The Emotional Impact of Watch and Wait for CLL. Available at: https://media.leukaemiacare.org.uk/wp-content/uploads/The-Emotional-Impact-of-Watch-and-Wait-for-CLL-EHA-2019-Poster.pdf. Last accessed 27.03.22
[37] Lymphoma Coalition. 2020 Global Patient Survey on Lymphomas & CLL. 2020. Available at: https://lymphomacoalition.org/wp-content/uploads/LC-2020-GPS-Global-Report-Final.pdf. Last accessed February 2023
[38] Khanijo, Sameer et al. “Thoracic complications in chronic lymphocytic leukemia.” Clinical Lymphoma Myeloma and Leukemia 17, no. 4 (2017): 220-224.
[39] Mauro, Francesca Romana et al. “Response to the conjugate pneumococcal vaccine (PCV13) in patients with chronic lymphocytic leukemia (CLL).” Leukemia 35, no. 3 (2021): 737-746.
[40] Arellano-Llamas, Abril Adriana et al. “Chronic Lymphocytic Leukemia in the SARS-CoV-2 Pandemic.” Current Oncology Reports (2022): 1-5.
[41] CLL Support. ‘Shingles’. Available at: https://www.cllsupport.org.uk/information-support/diagnosis/shingles-2/. Last accessed 08.03.23
[42] Morawska M. et al. Reasons and consequences of COVID-19 vaccine failure in patients with chronic lymphocytic leukemia. Eur J Haematol. 2022 Feb;108(2):91-98. doi: 10.1111/ejh.13722
[43] Antao, Nirav et al. “Herpes zoster in chronic lymphocytic leukemia: Effect of vaccination and treatment.” (2021): 7527-7527.
[44] Kumar, Abhishek et al. “Lumbar Erector Spine plane block for pain management in postherpetic neuralgia in a patient with chronic lymphocytic leukemia.” Indian Journal of Palliative Care 26, no. 1 (2020): 134.
[45] Vitale, Candida et al. “Autoimmune complications in chronic lymphocytic leukemia in the era of targeted drugs.” Cancers 12, no. 2 (2020): 282.
[46] Fattizzo, Bruno et al. “Autoimmune cytopenias in chronic lymphocytic leukemia: focus on molecular aspects.” Frontiers in Oncology 9 (2020): 1435.
[47] Tadmor, Tamar et al. “A review of the infection pathogenesis and prophylaxis recommendations in patients with chronic lymphocytic leukemia.” Expert Review of Hematology 11, no. 1 (2018): 57-70.
[48] Demir, Cengiz, and Ömer Ekinci. “Clinical and serological autoimmune complications in chronic lymphocytic leukemia.” Wiener klinische Wochenschrift 129, no. 15 (2017): 552-557.
[49] Tandra, Pavankumar et al. “Autoimmune cytopenias in chronic lymphocytic leukemia, facts and myths.” Mediterranean journal of hematology and infectious diseases 5, no. 1 (2013).
[50] Blood Cancer UK. Staying safe and government guidance. 2021. Available at: https://bloodcancer.org.uk/support-for-you/coronavirus-covid-19/looking-after-yourself-staying-home-shielding/. Last accessed February 2023
[51] Paneesha, Shankara et al. “Covid-19 infection in therapy-naive patients with B-cell chronic lymphocytic leukemia.” Leukemia research 93 (2020): 106366.
[52] Langerbeins, Petra, and Barbara Eichhorst. “Immune dysfunction in patients with chronic lymphocytic leukemia and challenges during COVID-19 pandemic.” Acta haematologica 144, no. 5 (2021): 508-518.
[53] Blood Cancer UK. How do you feel about lockdown easing? No date. Available at: https://bloodcancer.org.uk/support-for-you/coronavirus-covid-19/blood-cancer-and-coronavirus-stories/how-do-you-feel-about-lockdown-easing/. Last accessed February 2023
[54] Giesen, Nicola et al. Mellinghoff, Gernot Beutel, Catherina Lueck et al. “Evidence-based management of COVID-19 in cancer patients: Guideline by the Infectious Diseases Working Party (AGIHO) of the German Society for Haematology and Medical Oncology (DGHO).” European Journal of Cancer 140 (2020): 86-104.
[55] Lymphoma Coalition. COVID-19 resources. Available at: https://lymphomacoalition.org/covid-19-resources/. Last accessed February 2023
[56] European Society of Medical Oncology. COVID-19 vaccination. No date. Available at: https://www.esmo.org/covid-19-and-cancer/covid-19-vaccination. Last accessed February 2023
[57] Zheng, Guoqiao et al. “Types of second primary cancers influence survival in chronic lymphocytic and hairy cell leukemia patients.” Blood cancer journal 9, no. 4 (2019): 1-4.
[58] Mulligan, Stephen P et al. “Chronic lymphocytic leukemia, skin and other second cancers.” Leukemia & lymphoma 60, no. 13 (2019): 3104-3106.
[59] Ishdorj, Ganchimeg et al. “Risk factors for skin cancer and solid tumors in newly diagnosed patients with chronic lymphocytic leukemia and the impact of skin surveillance on survival.” Leukemia & lymphoma 60, no. 13 (2019): 3204-3213. ![]()
